Is Your Clinic in Compliance with Federal Regulations and State Statutes?

In mid-January, I learned that Fresenius Medical Care terminated 600 master’s prepared social workers (MSWs) and registered dietitians (RDs) who had been managers and supervisors for dialysis clinic social workers, dietitian, technical managers, and even some directors of operations. Previously, dialysis clinic social workers could rely on a professional colleague in their field to help and advise them in situations with patients, staff, or even management where they could benefit from a supervisor’s knowledge and experience. Some of the terminated professionals had decades of experience. In my opinion, this reorganization creates a tremendous brain drain that could have unintended consequences.
I am concerned that now dialysis clinic social workers and dietitians will have extremely high numbers of home and in-center patients, making it difficult to impossible to provide all of the services the federal regulations require. And, they will be relying on facility administrators (FAs) for supervision, when few FAs have training or experience as social workers or dietitians.
How to Avoid Citations
I am writing this blog to make sure that anyone who will be assuming
additional responsibility for assuring compliance with federal
regulations and state statutes and rules for scope of practice and
qualifications knows how to avoid citations. As a social worker, I plan
to focus  mostly
on federal and state rules and regulations that apply to social
workers’ qualifications and responsibilities to dialysis
patients.
mostly
on federal and state rules and regulations that apply to social
workers’ qualifications and responsibilities to dialysis
patients.
What follows are citations to the regulation text in the 2008 ESRD Conditions for Coverage (CfC) and the interpretation of those regulations for ESRD surveyors in the 2008 Interpretive Guidance (IG).1 It is important to read both the regulation text and the interpretation of those regulations to know what CMS expects to see when a dialysis clinic is surveyed and the “tag” the surveyor is to use to cite when a dialysis clinic is out of compliance. I will also share where to find the state rules and statutes that describe licensure requirements for social workers.
§ 494.140 Condition: Personnel qualifications states: “All dialysis facility staff must meet the applicable scope of practice board and licensure requirements in effect in the State in which they are employed. The dialysis facility’s staff (employee or contractor) must meet the personnel qualifications and demonstrated competencies necessary to serve collectively the comprehensive needs of the patients…”
CMS’ interpretation in the IG states: “All dialysis facility staff, including non-physician practitioners (whether employee, contractor, or credentialed as a member of the medical staff), must meet the applicable qualifications; scope of practice; and board and licensure requirements in effect in the State in which they are employed. All staff members are expected to practice within the licensure and/or certification requirements for their degree, practice setting, and scope of practice as defined by their individual State.” As stated in regulatory text and CMS interpretation of it, these requirements apply to all staff (employee or contract).
§ 42 CFR 494.140 Condition: Personnel qualifications states:
“(d) Standard: Social worker. The facility must have a social worker who—
 (1)
Holds a master’s degree in social work with a specialization in
clinical practice from a school of social work accredited by
the Council on Social Work Education; or
(1)
Holds a master’s degree in social work with a specialization in
clinical practice from a school of social work accredited by
the Council on Social Work Education; or
(2) Has served at least 2 years as a social worker, 1 year of which was in a dialysis unit or transplantation program prior to September 1, 1976, and has established a consultative relationship with a social worker who qualifies under § 494.140 (d)(1).”
CMS’ interpretation in the IG states: “Licensure requirements for master-prepared social workers in clinical practice vary from state to state. The masters (sic) prepared social worker must meet the licensure requirements in the state of practice.”
The role and responsibilities of the social worker can be found under the Conditions of Patient assessment and Patient plan of care as follows:
§ 494.80 Condition: Patient assessment
(a) Standard: Assessment criteria.
(7) Evaluation of psychosocial needs by a social worker.
CMS’ interpretation in the IG describes this in greater detail stating: “The evaluation of psychosocial needs must be conducted by a qualified social worker as defined by these regulations at V691.”
Examples of psychosocial parameters to be addressed by the qualified social worker include, but are not limited to:
Cognitive status and capacity to understand;
Ability to meet basic needs;
Ability to follow the treatment prescription;
Mental health history, capacities, and needs for counseling;
Substance abuse history, if any;
Current ability to cope with and adjust to dialysis;
Expectations for the future and living with kidney failure and treatment;
Educational and employment status, concerns, and goals;
Home environment including current living situation;
Legal issues ( e.g., court appointed guardian, advance directive status, and health care proxy)
Need for advocacy with traditional (nursing home) and non-traditional housing (e.g., homeless shelters, group homes);
Financial capabilities and resources;
Access to available community resources; and
Eligibility for Federal, State, or local resources.
The social worker is responsible for collaborating with the rest of the interdisciplinary team to address all clinical elements in the patient’s plan of care. However, psychosocial status is where it is intended for the qualified social worker to take the lead.
§ 494.90 Condition: Patient plan of care

(a) Standard: Development of patient plan of care. The interdisciplinary team must develop a plan of care for each patient.
(6) Psychosocial status. The interdisciplinary team must provide the necessary monitoring and social work interventions. These include counseling services and referrals for other social services, to assist the patient in achieving and sustaining an appropriate psychosocial status as measured by a standardized mental and physical assessment tool chosen by the social worker, at regular intervals, or more frequently on an as-needed basis.
CMS’ interpretation in the IG states in part: “To address the patient’s psychosocial needs and ‘achieve and sustain’ an appropriate psychosocial status, each patient's plan of care must reflect the information obtained from the applicable components of the IDT comprehensive assessment under the Condition for Patient assessment at V502-V515, including the psychosocial assessment at V510. The plan of care must include interventions individualized to meet that patient's psychosocial needs and aimed at optimizing the patient’s adjustment to kidney failure and its treatment. The social worker is expected to assist patients in achieving their psychosocial goals. Counseling services to patients and their families should be directed at helping the patient and family cope with kidney failure and dialysis, follow the treatment plan, and achieve the patient’s goals for rehabilitation…”
An important requirement in the ESRD CfC is under the Condition for Governance and relates to sufficient staffing for all disciplines to meet patients’ clinical needs.
§ 494.180 Condition: Governance
“(b) Standard: Adequate number of qualified and trained staff. The governing body or designated person responsible must ensure that--
(1) An adequate number of qualified personnel are present whenever patients are undergoing dialysis so that the patient/staff ratio is appropriate to the level of dialysis care given and meets the needs of patients; and The registered nurse, social worker and dietitian members of the interdisciplinary team are available to meet patient clinical needs;”
CMS’ interpretation in the IG states: “The governing body is expected to make diligent efforts to promptly fill vacant positions. If the nurse manager, social worker, dietitian or other required or necessary position is vacant for more than a month, the governing body must make some provision for temporary coverage. If the facility “shares” the social worker or dietitian with multiple clinics or requires professional staff to perform non-clinical tasks, it must not negatively impact the time available to provide the clinical interventions required to achieve the goals identified in the patient’s plan of care. The facility CEO or administrator is responsible to assure the professional support staff members have sufficient time available in the facility to meet the clinical needs of in-center and home dialysis patients.”
State Licensure for Social Workers
The National Association of Social Workers’ Standards of Practice in Health Care Settings states under Definitions: “Within the United States, a social worker is an individual who possesses a baccalaureate or master’s degree in social work from a school or program accredited by the Council on Social Work Education. Although all 50 states and the District of Columbia license or certify social workers, licensure and certification laws vary by state. Each social worker should be licensed or certified, as applicable and required, at the level appropriate to her or his scope of practice in the practitioner’s jurisdiction(s).”2
Both the social worker and facility administrator must be sure the social worker’s license covers the scope of practice described in the ESRD CfC, which includes meeting the applicable scope of practice board and licensure requirements in effect for the State in which they are employed and providing counseling under the Patient Plan of Care at 42 CFR 494.90(a)(6). Some states allow a licensed master social worker to provide counseling, but in others, a licensed master social worker providing counseling must be supervised by a clinical social worker or have a clinical social work license.
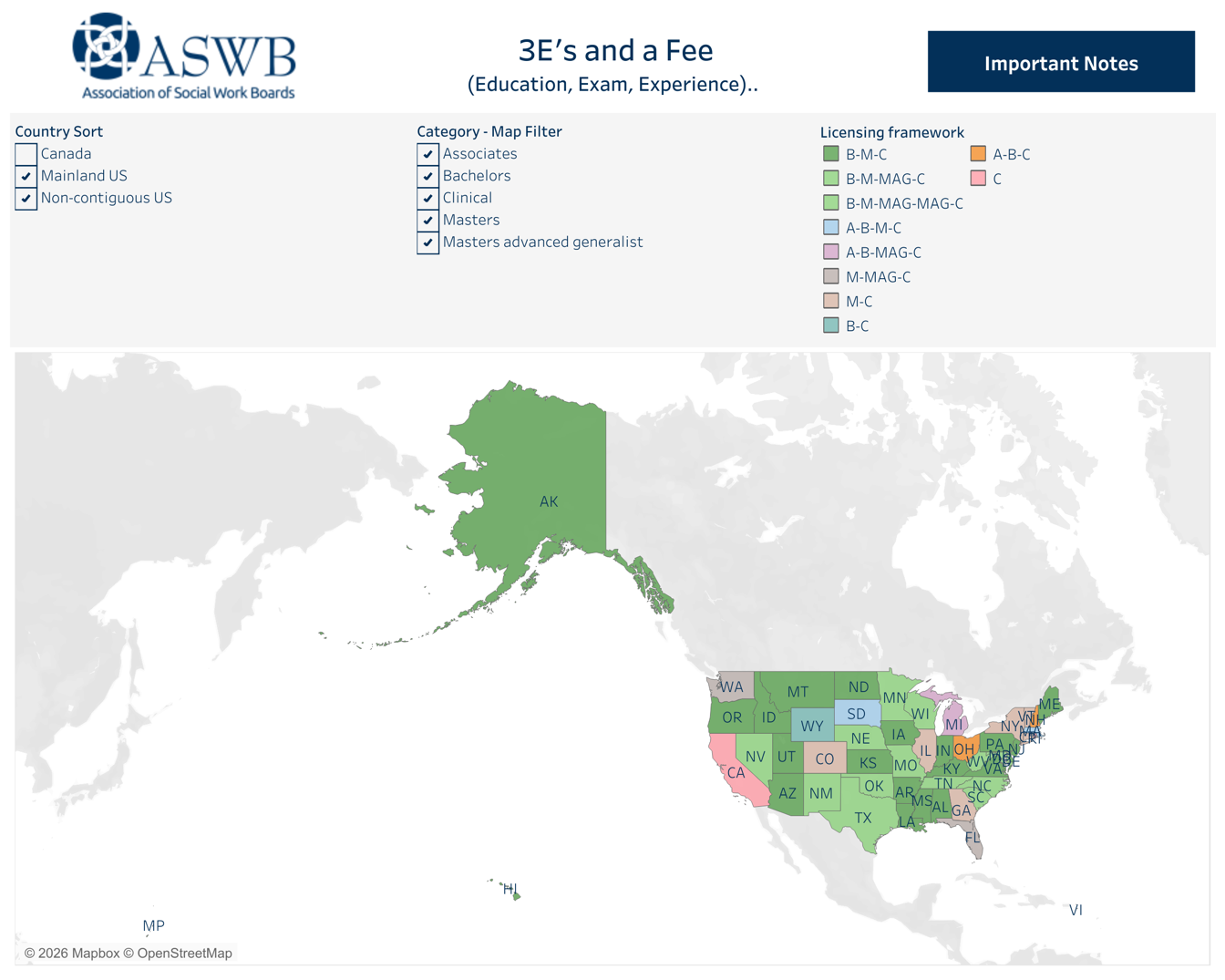
To know what license is required, social workers and dialysis facility administrators can refer to the Association of Social Work Boards (ASWB), which states, “The purpose of licensing in social work is to protect the public by setting and enforcing standards for social work practice.” ASWB, a nonprofit organization of state regulatory boards and colleges, developed and administers the most commonly used standardized licensing exams for all levels of social work licensure and offers online trainings, sample tests, and a guidebook to help social workers prepare for an exam.
States may have multiple levels of social work licensure. In jurisdictions that have title and/or practice act protection, only licensed social workers are permitted to call themselves a social worker and practice social work. ASWB has a color-coded map. Click on any state to see levels of licensure/registration in that state. “Important Notes” state what the letters stand for on that map.3 The ASWB site links to social work licensing boards where a social worker’s license can be verified.4
The Social Work Licensure Compact is expected to be implemented soon, which will allow a social worker who is licensed or eligible for a social work license and living in a compact state to apply for a multistate license to practice in another compact state.5 This should help dialysis providers that have clinics in multiple states and reduce the licensure burden on social workers who practice across state lines.
Why All This Matters
It’s easy for those working in dialysis who have worked with many patients to forget the impact a chronic life-altering disease can have on a home or in-center dialysis patient. Yet, patients who dialyze at home or in-center can’t ignore the burden or forget the tenuousness of life. As a result, dialysis patients may be anxious, angry, and depressed. Many have financial stress due to challenges with energy levels, treatment schedules, and/or the high cost of care that may not be fully covered by insurance and changes in employment status.

The USRDS 2025 Annual Data Report states in Table 1.4 that in 2023, 51.5% of patients on in-center HD, 37% of those on home HD, and 29% of those on PD had the highest social deprivation index (SDI) scores: 67-100.6 It is no wonder these patients need help with challenging psychosocial problems that experienced dialysis social workers with sufficient staffing can address. If a patient-to-social worker ratio is too high, limiting the time social workers have to address these problems, psychosocial problems may contribute to patients’ failure to follow their treatment plan and poor outcomes for clinical measures may result in loss of Medicare revenue.
I believe that having social workers supervised by social workers with acuity-based ratios and assigned only to do tasks within their license’s scope of practice could go a long way toward achieving the outcomes clinics want to achieve and the goals that patients desire. It may be illuminating to compare outcomes in clinics that still have area lead social workers supervising clinic social workers with those that have social workers supervised by facility administrators. If it makes a difference, social workers and patients deserve nothing less.
Centers for Medicare & Medicaid Services (2008). ESRD Surveyor Training Interpretive Guidance Final Version 1.1. https://www.cms.gov/medicare/provider-enrollment-and-certification/guidanceforlawsandregulations/downloads/esrdpgmguidance.pdf↩︎
NASW Standards for Social Work Practice in Health Care Settings (2016). https://www.socialworkers.org/Practice/NASW-Practice-Standards-Guidelines/NASW-Standards-for-Social-Work-Practice-in-Health-Care-Settings↩︎
ASWB (2022). Licensing requirements by state or province. 3 Es and a Fee (Education, Exam, Experience). https://www.aswb.org/licenses/how-to-get-a-license/licensing-requirements-by-state-or-province/↩︎
ASWB. Look up a license. https://www.aswb.org/licenses/protecting-the-public/look-up-license/↩︎
Social Work Compact map. https://swcompact.org/compact-map/↩︎
United States Renal Data System. 2025 USRDS Annual Data Report: Epidemiology of kidney disease in the United States. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, Bethesda, MD, 2025. https://usrds-adr.niddk.nih.gov/2025/end-stage-renal-disease/1-incidence-and-prevalence↩︎
Comments
Susie Payne
Jan 29, 2026 10:30 PM
I think too many social workers, both new hires and ones who have been about a while, don't understand and/or value the expertise and knowledge one can gain from belonging to our professional organizations. Since I am part of an LDO (large dialysis organization), we are very likely in compliance with the regulations you noted. We have regional lead social workers and they do a good job. But every clinic is different, with different pt needs and concerns, and I am not sure those acuity levels are taken into consideration in relation to social work staffing ratios and the work that needs to get done well to meet pt needs. Thanks again for the work you - and others - do to keep our organization strong and relevant!